
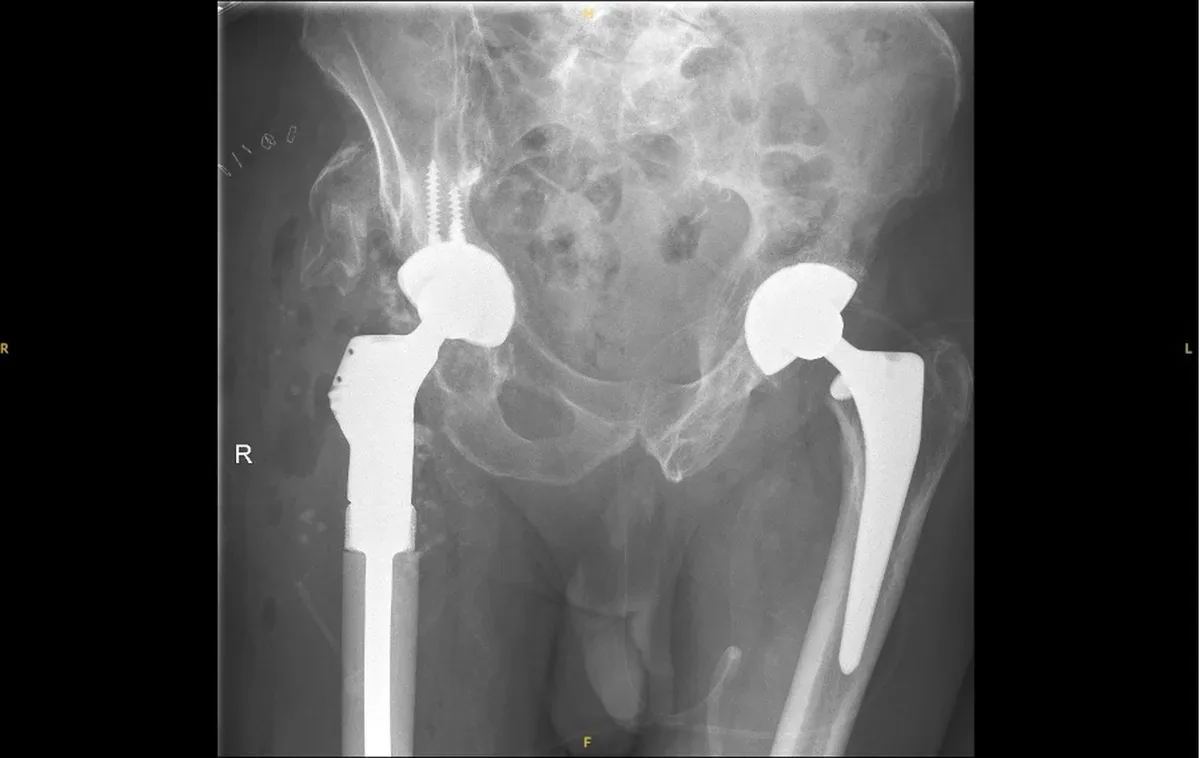
The single most important distinction between the two operations is what happens to the upper end of the femur. In a total hip replacement, the femoral head is removed entirely and a metal stem is inserted into the shaft of the femur. The stem anchors the new ball-and-socket joint; the upper femur is essentially bypassed. In hip resurfacing, the head is preserved. The arthritic surface is trimmed and capped with a metal or ceramic shell; the femoral neck and head remain intact, and the stem is short, extending only a few centimetres into the neck.
This distinction in bone preservation is the reason some patients and surgeons prefer resurfacing when the anatomy is suitable. A patient who undergoes resurfacing retains the femoral head and neck in their natural state; if the implant ever needs to be replaced, the revision operation proceeds from a preserved, near-normal femur rather than one that has had its head removed and its canal occupied by a stem for many years. The practical significance of this depends heavily on how old the patient is at primary surgery and how long the original implant lasts.
Total hip replacement, by contrast, is anatomically versatile. It works equally well in patients with large or small femoral heads, in those with significant bone loss from osteonecrosis or dysplasia, and in any age group. The range of patients who are anatomically suitable is considerably wider.

A resurfacing bearing closely matches the diameter of the patient's own femoral head, typically between 44 mm and 56 mm in adults. This large bearing surface is one of resurfacing's mechanical advantages: a larger ball is significantly harder to dislocate than a smaller one. The historic dislocation rate after primary total hip replacement, with its smaller ball and resected soft-tissue envelope, has been a genuine clinical problem; more recent techniques (larger femoral heads, dual-mobility cups, improved surgical approaches) have reduced but not eliminated this risk. Resurfacing, by retaining the native head diameter, avoids it almost entirely.
In the original metal-on-metal era, the large bearing also meant a large contact area for cobalt-chromium wear debris, which contributed to the problems described on the metallosis page. The two newer ceramic resurfacing systems, the ReCerf and the H1, replace the metal-on-metal bearing with ceramic-on-ceramic, retaining the stability advantage while removing the source of metal ion release. These systems are discussed in detail on the implants page.
Total hip replacement uses a variety of bearing combinations: metal or ceramic head on a polyethylene or ceramic liner. Modern highly cross-linked polyethylene has excellent wear characteristics and is now the most commonly used liner material in the UK. Ceramic-on-ceramic bearings in total hip replacement are also established, with very low wear and a long track record. Neither is inherently superior to the other across all patients; bearing choice in both operations depends on anatomy, age, activity, and surgeon experience.

Registry data are the most reliable guide to implant longevity because they capture outcomes across the full range of surgeons and hospitals, not just specialist centres. The National Joint Registry (NJR) for England, Wales, Northern Ireland and the Isle of Man is the largest arthroplasty registry in the world and publishes annual reports covering hundreds of thousands of procedures.
For total hip replacement, the picture is well-established: modern cementless and cemented constructs show ten-year revision rates in the range of 4–6% in most age groups, with twenty-year data available for many designs. Longevity is generally better in older patients, in whom lower activity levels reduce mechanical demands on the implant.
For hip resurfacing, the data are more nuanced. The Adept metal-on-metal implant has the longest UK registry record of any resurfacing system, with ten-year revision rates of around 3–5% in large-head male patients: comparable to, and in some series better than, total hip replacement in the same group. These results are, however, strongly patient-dependent: women, patients with smaller native heads, and those with anatomical risk factors have historically had higher revision rates with metal resurfacing. The newer ceramic systems, ReCerf and H1, have promising two- and five-year outcomes but do not yet have the decades of follow-up available for total hip replacement. Building that evidence base is an active priority in hip surgery research.
Longevity data should be read in the context of who the operation was performed on. A ten-year survival figure for resurfacing drawn from a mixed population including high-risk subgroups will look worse than one drawn from an optimally selected series. This is one reason why surgeon volume and patient selection both matter, and why the conversation about which operation is right for an individual patient is more useful than an abstract comparison of headline survival rates.
Patients who undergo hip resurfacing typically return to higher levels of physical activity than those who undergo total hip replacement, but the comparison requires care. Part of the difference reflects selection: resurfacing candidates tend to be younger, fitter, and more motivated to return to sport than the average patient who undergoes a total hip replacement. Part reflects genuine biomechanical differences.
Resurfacing preserves the femoral head and neck, and with them the normal loading pattern through the proximal femur. This is thought to reduce the risk of stress shielding, the remodelling of bone that can occur when a femoral stem transfers load differently from the native anatomy. Whether this translates into superior long-term function in randomised trials has been debated; several studies show equivalent Oxford Hip Score outcomes between the two operations when patients are matched for age and activity level. What is clearer is that the large bearing and lower dislocation risk of resurfacing give some patients greater confidence in high-demand activities such as hiking, cycling, skiing and impact sports.
Total hip replacement is routinely performed in patients who wish to return to activity, and many do so successfully. Most surgeons advise against high-impact repetitive loading (running, jumping sports) in the long term, on the grounds of accelerated bearing wear and periprosthetic bone stress. These restrictions tend to be applied to resurfacing patients as well, with the exception that impact loading through a preserved femoral neck is considered more physiological than loading through a femoral stem. In practice, activity guidance is individualised according to bearing type, implant fixation, bone quality, and the patient's own goals.

Total hip replacement is suitable for almost everyone with a painful arthritic hip who has not responded to non-operative treatment. It can be performed in patients with small femoral heads, osteopenic bone, previous hip surgery, avascular necrosis, severe dysplasia, and in any age group. It is the default operation for most patients presenting with end-stage hip disease.
Hip resurfacing requires specific anatomy. The femoral head must be large enough to accommodate a cap, the bone quality must be sufficient to support the implant, and the neck-shaft angle must be within a range that permits safe component positioning. In the metal-on-metal era, the practical effect of these requirements was that resurfacing was most reliably offered to men with a head diameter above approximately 48 mm, good bone density, and no significant acetabular dysplasia.
The arrival of ceramic-on-ceramic resurfacing, releasing no metal ions and suitable across the range of native head sizes, has begun to reopen resurfacing as an option for some patients previously excluded, including women and those with more modest head dimensions. This development, and its implications for candidacy, is covered in detail on the hip resurfacing for women and Am I a candidate? pages. The anatomy question is now less binary than it was a decade ago, but it remains one of the most important variables in the decision.
MRI scanning after hip surgery is complicated by metal implants, which distort the magnetic field and degrade image quality around the joint. This is a practical consideration for patients who may need pelvic or lumbar spine imaging in future, or who have a condition that requires regular cross-sectional surveillance.
Both operations involve metal components and both produce MRI artefact to some degree. Metal-on-metal hip resurfacings have historically produced the most severe artefact, in part because the large metal-on-metal bearing creates a large zone of signal distortion. Specialised MARS-MRI sequences can reduce this artefact and are routinely used in the surveillance of metal-on-metal implants, but image quality remains inferior to a native hip.
Ceramic resurfacing implants produce less metal artefact than metal-on-metal designs, for the simple reason that only the fixation components (the short femoral peg and the cup shell) contribute metallic signal distortion; the bearing surfaces themselves are ceramic. Modern total hip replacements with ceramic-on-polyethylene or ceramic-on-ceramic bearings have a similar profile. Neither operation renders MRI impossible, but both introduce some limitation on the clarity of imaging in and around the hip joint. For patients with known conditions requiring regular abdominal or pelvic MRI, this is worth discussing before surgery.
Every hip implant may eventually require revision, and the ease of that revision is partly determined by what was done at the primary operation. This is one of the most cited arguments in favour of resurfacing in younger patients.
When a hip resurfacing fails, whether from aseptic loosening, component malposition, adverse reaction to metal debris (in metal-on-metal implants), or fracture of the femoral neck, the revision operation proceeds from an intact femoral head and neck. The surgeon removes the cap and cup, and typically implants a standard total hip replacement. Because the femoral canal has not been filled with a primary stem, there is no stem extraction and the structural bone stock of the upper femur is preserved. Published series of resurfacing revisions generally report outcomes comparable to those of primary total hip replacement, provided revision is undertaken before significant bone or soft-tissue damage has developed.
Revision of a total hip replacement is a more demanding operation. The femoral stem must be extracted, a procedure that can range from straightforward to technically complex depending on the degree of osseointegration, stem design, and the reason for revision. There may be bony defects in both the femur and acetabulum that require augmentation, impaction grafting, or custom components. Recovery is generally longer than for a primary hip replacement, and the re-revision rate over ten years is higher than for primary procedures. These considerations are not arguments against total hip replacement (the vast majority of patients never require revision), but they do inform the logic of the original choice in younger patients where revision is more likely to occur within the patient's lifetime.
A quick-reference overview of the key differences. The right choice for any individual depends on anatomy, age, activity goals, and the bearing options that are appropriate for their specific situation.
| Factor | Hip Resurfacing | Total Hip Replacement |
|---|---|---|
| Femoral boneUpper femur | Head and neck preserved; arthritic surface reshaped and capped | Head excised; stem seated in the femoral canal |
| Bearing size | Near-native head diameter (typically 44–56 mm) | Smaller fixed head size (historically 28–36 mm; modern designs up to 40 mm) |
| Dislocation risk | Very low; large bearing is inherently stable | Low with modern technique; higher with smaller heads and posterior approach |
| Bearing materialModern options | Metal-on-metal (Adept); ceramic-on-ceramic (ReCerf, H1) | Ceramic or metal head on cross-linked polyethylene or ceramic liner |
| Metal ion risk | Present with metal-on-metal bearings; eliminated with ceramic resurfacing | Taper corrosion possible but bearing surface risk low with ceramic/polyethylene |
| MRI artefact | Moderate; least with ceramic bearings | Moderate; depends on stem and bearing material |
| Anatomical rangeWho qualifies | Requires sufficient head size and bone quality; expanding with modern ceramic designs | Almost any anatomy; suitable for all head sizes and bone qualities |
| Activity level | High-demand activity typical in registry populations; good data for sport return | Activity return common; some surgeons counsel against high-impact repetitive sport |
| LongevityRegistry data | Comparable to THR in optimal patients; long-term ceramic data still accumulating | Well-established; 10-year revision rates 4–6%; 20-year data available for many designs |
| If revision needed | Converts to standard THR on intact femur; generally straightforward | Stem extraction required; technically more demanding; bone defects common |
| Typical patient | Active adults with sufficient anatomy; classically younger men; now expanding | Any patient with end-stage hip disease; the default operation for most |
Hip resurfacing uses a bearing close to the size of your natural femoral head, which makes dislocation rare. Total hip replacement uses smaller head sizes, and although modern techniques have reduced the risk considerably, dislocation remains one of its more common early complications. For patients whose work or sport involves extreme hip positions, this difference can be a deciding factor.
On the femoral side, yes. Because resurfacing preserves the femoral head and neck, a failed resurfacing usually converts to a standard primary hip replacement on intact bone. Revising a total hip replacement means removing the existing stem, which is a bigger undertaking and often involves some bone loss. This is one of the main reasons younger patients consider resurfacing first.
The early weeks are broadly similar: both operations have most patients walking on the day of surgery and off crutches within about six weeks. The difference shows later. Well-selected resurfacing patients are typically cleared for a graduated return to impact sport from four to six months, a level of activity most surgeons discourage after a total hip replacement. The full timeline is on the recovery page.
Three reasons. Suitability is genuinely narrower: the operation needs good bone quality and suitable anatomy. The metal-on-metal era made many surgeons wary, and most stopped offering the operation entirely. And it is a technically demanding procedure concentrated in a small number of high-volume specialist units, so many patients are simply never told it is an option. How suitability is assessed is on the candidacy page, and what to look for in a surgeon is covered in choosing a hip resurfacing surgeon.
Some patients do, but most surgeons advise against regular impact sport on a total hip replacement because of wear and loosening concerns. Resurfacing was designed with impact activity in mind, and a return to running is a realistic goal for well-selected resurfacing patients; the phased return is mapped in the guide to running after hip resurfacing.
The decision between resurfacing and replacement turns on individual anatomy, bone quality, age and activity goals. A consultation includes a review of imaging, a discussion of your expectations, and a clear recommendation based on what the evidence supports for your specific situation. Fixed self-pay packages and insurer details are on the fees page.
Book a Consultation Am I a Candidate?